Bfr Training Elderly Vascular - BFR Training
Up One Level
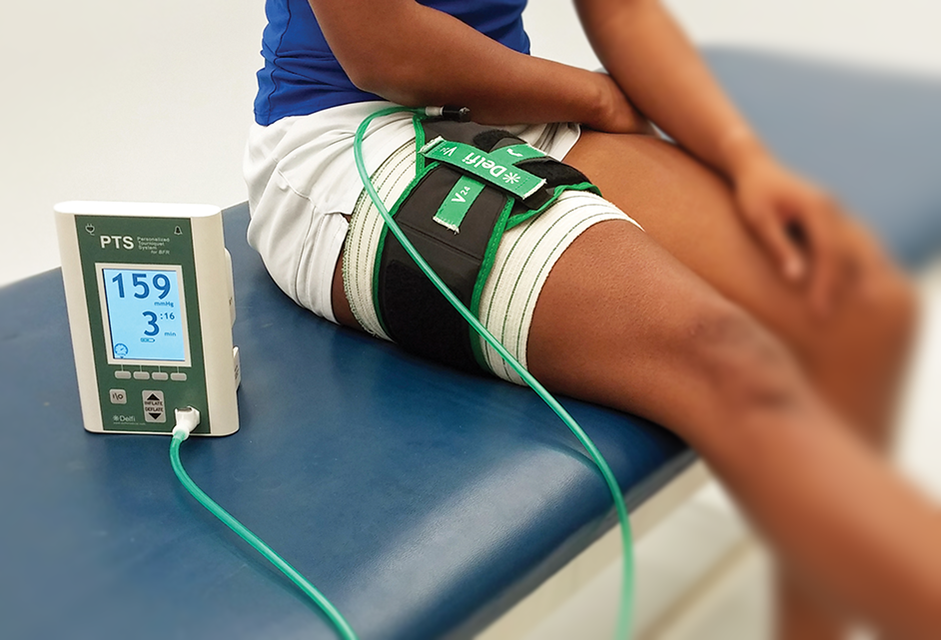
What Is Bfr Training
It can be used to either the upper or lower limb. The cuff is then inflated to a particular pressure with the objective of getting partial arterial and complete venous occlusion. blood flow restriction physical therapy. The patient is then asked to carry out resistance workouts at a low intensity of 20-30% of 1 repeating max (1RM), with high repetitions per set (15-30) and short rest intervals between sets (30 seconds) Comprehending the Physiology of Muscle Hypertrophy. Muscle hypertrophy is the increase in size of the muscle along with a boost of the protein content within the fibres.
Myostatin controls and inhibits cell growth in muscle tissue. It needs to be essentially closed down for muscle hypertrophy to take place. does blood flow restriction training work. Resistance training results in the compression of capillary within the muscles being trained. This causes an hypoxic environment due to a decrease in oxygen delivery to the muscle.
( 1) Low intensity BFR (LI-BFR) results in an increase in the water content of the muscle cells (cell swelling). It also speeds up the recruitment of fast-twitch muscle fibers - what is bfr training. It is likewise hypothesized that when the cuff is removed a hyperemia (excess of blood in the blood vessels) will form and this will trigger further cell swelling.
A wide cuff is preferred in the proper application of BFR. 10-12cm cuffs are normally used. A large cuff of 15cm may be best to enable even limitation. Modern cuffs are formed to fit the natural shape of the arm or thigh with a proximal to distal constricting. There are likewise specific upper and lower limb cuffs that permit better fitment.
The narrower cuffs are normally flexible and the broader nylon. With elastic cuffs there is a preliminary pressure even before the cuff is inflated and this leads to a different ability to limit blood circulation as compared to nylon cuffs. Elastic cuffs have actually been revealed to provide a considerably greater arterial occlusion pressure instead of nylon cuffs - bfr training.
g. 180 mm, Hg; a pressure relative to the patient's systolic high blood pressure, for e. g. 1. 2- or 1. 5-fold greater than systolic blood pressure; a pressure relative to the patient's thigh circumference. It is the best to use a pressure specific to each specific client, due to the fact that different pressures occlude the amount of blood flow for all individuals under the very same conditions.
How Does Blood Flow Restriction Weight Training Work
The cuff is inflated to a specific pressure where the arterial blood circulation is completely occluded. This known as limb occlusion pressure (LOP) or arterial occlusion pressure (AOP). The cuff pressure is then computed as a portion of the LOP, usually between 40%-80%. Utilizing this method is more effective as it ensures clients are working out at the appropriate pressure for them and the kind of cuff being utilized.
BFR-RE is generally a single joint workout technique for strength training. Muscle hypertrophy can be observed during BFR-RE within a 3 week duration however a lot of studies advocate for longer training durations of more than 3 weeks. A load of 20-40% 1RM has been revealed to produce constant muscle adjustments for BFR-RE.
An organized review carried out by da Cunha Nascimento et al in 2019 analyzed the long and short-term effects on blood hemostasis (the balance in between fibrinolysis and coagulation). It concluded that more research study needs to be performed in the field prior to definitive guidelines can be provided. In this evaluation, they raised issues about the following Adverse impacts were not always reported The level of previous training of subjects was not shown which makes a substantial distinction in physiological action Pressures applied in research studies were exceptionally variable with various approaches of occlusion in addition to requirements of occlusion The majority of studies were conducted on a short-term basis and long term actions were not determined The studies concentrated on healthy topics and exempt with danger for thromboembolic disorders, impaired fibrinolysis, diabetes and obesity Their final conclusion on the safety of BFR was as such: In general, it is well developed that unaccustomed exercise results in muscle damage and delayed beginning muscle soreness (DOMS), especially if the exercise includes a large number of eccentric actions. bfr training dangers.
As your body is healing after surgery, you might not have the ability to position high stresses on a muscle or ligament. Low load exercises may be needed, and blood flow constraint training permits optimum strength gains with minimal, and safe, loads. Performing BFR Training Prior to starting blood circulation constraint training, or any exercise program, you must inspect in with your doctor to guarantee that workout is safe for your condition (bfr training chest).
Launch the contraction. Repeat gradually for 15 to 20 repetitions. Your physical therapist may have you rest for 30 seconds and after that repeat another set. Blood circulation limitation training is supposed to be low strength however high repeating, so it is common to carry out two to 3 sets of 15 to 20 representatives during each session.
Who Should Refrain From Doing BFR Training? People with specific conditions should not engage in BFR training, as injury to the venous or arterial system may happen. Contraindications to BFR training might include: Before carrying out any exercise, it is essential to consult with your physician and physical therapist to ensure that exercise is right for you.
Why Is Bfr Training Effective For Improving Muscle Strength And Mass
Over the last number of years, blood circulation limitation training has gotten a great deal of favorable attention as an outcome of the incredible boosts to size & strength it offers. However numerous people are still in the dark about how BFR training works. Here are 5 essential tips you should understand when beginning BFR training.
There are a number of different tips of what to use floating around the internet; from knee covers to over-sized rubber bands (blood flow restriction training). To make sure as precise a pressure as possible when carrying out practical BFR training, we recommend function developed solutions like our Bf, R Pro ARMS & Bf, R Pro LEGS straps.
Some studies recommend to increase efficiency of your fast-twitch fibers (those for explosive power and strength) you should raise around 40% of your 1RM. Adjust Your Representatives and Rest Periods Whilst you are going to be lowering the strength of weight you're lifting; you're going to be upping the intensity and volume of your exercise.
It's essential that you adjust your recovery appropriately but compared to heavy lifting then there is less muscle damage when doing low load BFR training. Studies have revealed that no increases in muscle damage continue longer than 24 hours after a BFR exercise suggesting it is safe to be performed every other day at most; however the best gains in muscle size and strength have actually been found carrying out 2-3 sessions of BFR per week. Do be mindful, nevertheless, if you are just beginning blood circulation constraint training or are unaccustomed to such high-repetition sets, you might need a little longer to recuperate from such metabolically requiring training.
005) was observed only in the HIIT group. Both, GH and IGF-1 increased significantly right away after the interventions, however without differences in between groups (no interaction effect). La increased during the intervention in a comparable way among both groups. Conclusions The combined intervention effectively improves the optimum power in context of endurance capability.
The improved HIF-1 in the HIIT+BFR as compared to the HIIT recommends that the combined intervention may have a remarkable physiological stimulus. Based upon the presented theoretical background and the insights of the investigation by Taylor, et al. , the function of this study was to examine the impacts of a HIIT in combination with BFR (utilizing KAATSU-cuffs) in comparison to a sole HIIT on physical performance.
Athletes Who Use Bfr Training
It is to be presumed that this intervention results in greater metabolic stress, which might catalyze adaption processes in this context. To clarify the degree of metabolic stress, the build-up of blood lactate concentrations (La) throughout the intervention as well as acute and basal modifications of the GH and IGF-1 have been measured (blood flow restriction training).
Study style The groups BFR+HIIT and HIIT carried out a HIIT-intervention for 4 weeks, three times weekly (Monday, Wednesday, Friday). Instantly prior to each HIIT-intervention, 4 sets of deep squats without extra load were carried out by both groups. The BFR+HIIT group performed the deep squats under BFR conditions. Within one week before (pre) and after (post) of the four-week intervention, the endurance capability was checked utilizing a spiroergometry on a bicycle-ergometer.
The GH and IGF-1 were evaluated immediately prior to and after the first (T1, T2) and last (T3, T4) intervention to measure acute (T1 to T2 and T3 to T4) and basal (T1 to T3) changes. Throughout the sixth intervention, the La were determined instantly prior to (pre) and after the BFR/squat (post BFR/squat) and after the HIIT (post HIIT).
This was performed on bicycle-ergometers (Kardiomed, Bike, Proxomed, Germany) and included three intervals each enduring 4 minutes with a resting duration of one minute. The intervals were performed with an intensity which was gotten used to the second ventilatory threshold plus 5 percent (BFR+HIIT HR: 168 14 min-1 ; HIIT HR: 163 15 min-1 , with heart rate (HR) as the control parameter (determined by the heart rate display FT7, Polar, Finland). This strength was picked due to the fact that of the requirement that a HIIT should be performed at an intensity greater than the anaerobic limit
For the pre-post contrast, the main worths of the height of the three CMJ were determined. The 1RM was determined using the multiple repetition optimum test as explained by Reynolds, et al. The test was assessed with the workout dynamic leg press. Diagnostics of metabolic stress/growth factors Blood samples were gathered by a medical physician at the above-mentioned time points (T1, T2, T3, T4) from a shallow forearm vein under stasis conditions.
Blood Flow Restriction Training How To
The blood samples were examined in a regional medical laboratory. La was measured on the ear lobe of the individuals to the time points as discussed in the study style. The samples were evaluated with the determining device Super GL3 by HITADO (Germany; determining error < 1. 5% according to the producer's details).
For generally dispersed data, the interaction impact between the groups over the intervention time was contacted a two-way ANOVA with repeated measures (elements: time x group). Afterwards, distinctions in between measurement time points within a group (time effect) and distinctions in between groups during a measurement time point (group result) were analysed with a dependent and independent t-test.
Therefore, the groups can be thought about homogeneous at the start of the intervention. Table 1: Mean values (basic deviation) of criteria of endurance and strength performance collected in the pre- and post-test in the BFR+HIIT group and HIIT group. View Table 1 After the 4 weeks of intervention, we figured out a substantial increase in the maximal power in both groups with the boost in the BFR+HIIT group being approximately two times as high as in the HIIT group (see interaction impact in Table 1).
In the BFR+HIIT group, the increase in power during the VT1 was much higher than in the HIIT (see Table 1). These outcomes did not end up being statistically considerable but for the BFR+HIIT group, a propensity (0. 100 > p > 0. 050) was observed. The improvements can be thought about almost relevant.
While the BFR+HIIT group was able to boost their power with continuous HR (describing the VT2 + 5%, see approaches) to + 8. 5% (1. to 2. week, p < 0. 001), + 8. 9% (2. to 3. week, p < 0. 001) and + 4 (blood flow restriction cuffs). 0% (3. to 4.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5609669/
RS
SSL Active
What does blood flow restriction training do?
https://www.menshealth.com/fitness/a19534758/blood-flow-restriction-to-build-muscle/
SSL Active
What does BFR stand for in exercise?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6530612/
SSL Active
Does BFR training hurt?
https://www.sportsinjurybulletin.com/blood-flow-restriction-training-feel-the-pressure/
SSL Active
How often should I do BFR training?
https://www.physio-pedia.com/Blood_Flow_Restriction_Training
SSL Active
Does BFR training increase size?
https://www.forbes.com/sites/leebelltech/2019/03/30/smart-cuffs-how-blood-flow-restriction-training-is-the-next-big-fitness-trend/
SSL Active
Does BFR training increase strength?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6683630/
SSL Active
Are BFR bands dangerous?
BFR works through the partial occlusion of blood flow. According to multiple research studies, WIDER CUFFS DECREASE THE PRESSURE NEEDED TO RESTRICT BLOOD FLOW. This means that the small cuffs sold by many “BFR” manufacturers increase the risk of soft tissue damage.
https://thebarbellphysio.com/blood-flow-restriction-training-safe/
SSL Active
Who benefits from BFR training?
https://www.issaonline.com/blog/index.cfm/2020/blood-flow-restriction-training-what-trainers-need-to-know
SSL Active
What is the ideal BFR?
https://precisionhealthclinics.com.au/bfr-what-the-heck-is-it/
SSL Active
What are the benefits of BFR bands?
https://bstrong.training/blogs/articles/blood-flow-restriction-training-benefits
SSL Active
Do BFR bands really work?
https://www.onnit.com/academy/is-it-legit-occlusion-training-for-muscle-growth/
SSL Active
How does BFR build muscle?
Elastic BFR bands partially restrict the venous blood (oxygen deficient blood flowing from the limbs back to the heart) return. This makes the muscles work even harder to pump the blood back to the heart!Nov 13, 2020
https://www.athletico.com/2020/11/13/how-does-blood-flow-restriction-work/
SSL Active
How long can you keep BFR bands on?
https://www.bfrbands.com/faqs/
SSL Active
Can I do occlusion training everyday?
https://www.bfrbands.com/is-it-bad-to-do-the-same-exercise-every-day/
SSL Active
Does BFR work for chest?
https://pubmed.ncbi.nlm.nih.gov/20618358/
SSL Active
Where do you put your BFR band for your butt?
https://recoverfun.com/blogs/blood-flow-restriction-training/how-to-use-bfr-training-to-grow-your-arms-legs-and-booty
SSL Active
How do you program BFR training?
- The generally prescribed protocol is as follows: ...
- Set 1: 30 reps / Rest: 30-60 seconds.
- Set 2: 15 reps / Rest: 30-60 seconds.
- Set 3: 15 reps / Rest: 30-60 seconds.
- Set 4: 15 reps / Rest: 30-60 seconds. ...
- Barbell Bench Press 80-85% 1RM.
https://drjohnrusin.com/blood-flow-restriction-scientifically-advancing-muscular-strength-hypertrophy/
SSL Active
How tight should occlusion bands be?
https://www.bfrbands.com/tips-for-using-occlusion-training-wraps-effectively/
SSL Active
Does blood flow help muscle growth?
https://www.phd.com/perform-smart/the-importance-of-a-muscle-pump-for-increased-muscle-growth/
SSL Active
Does BFR increase HGH?
https://www.precisionpt.org/post/blood-flow-restriction-training-deserving-the-hype
SSL Active
How can I get huge muscles?
- Eat Breakfast to help build Muscle Mass. ...
- Eat every three hours. ...
- Eat Protein with Each Meal to Boost Your Muscle Mass. ...
- Eat fruit and vegetables with each meal. ...
- Eat carbs only after your workout. ...
- Eat healthy fats. ...
- Drink water to help you build Muscle Mass. ...
- Eat Whole Foods 90% of The Time.
https://www.everyoneactive.com/content-hub/gym/eight-tips-help-build-muscle-mass/
SSL Active
Can you use BFR bands while running?
https://pure-physio.com/endurance-bfr-training/
SSL Active
Can BFR training cause blood clots?
Research from surgical tourniquet tells us that complete vascular occlusion can cause the formation of a thrombus (blood clot). The incidence rate of suffering a venous thrombosis during BFR training is 0.06%, and this number is lower than the general population figure.
https://sujibfr.com/blogs/blog/is-blood-flow-restriction-training-safe
SSL Active
What are the best BFR bands?
- BFR Bands. Occlusion Training Bands. ...
- Superpump! Kaatsu-inspired Training Straps. ...
- Ronin Wraps. BFR Occlusion Bands (4 pack) ...
- Beast Pump. Occlusion Bands (4 pack) ...
- Lifting Lab. Ultimate Arm Builder.
https://bestreviews.com/best-occlusion-training-bands
SSL Active
Does BFR increase vascularity?
BFRT increases vascularity and allows you to build more strength from lighter loads. This allows you to do more repetitions. You may only need to use weights that are 20 percent of your normal weight.Sep 13, 2019
https://www.healthline.com/health/veiny-arms
SSL Active
001) along with general to + 23. 7% (1. to 4. week, p < 0. 001), the improvement of the power in the HIIT group was just + 5. 3% (1. to 2. week, p = 0. 049), + 5 (is blood flow restriction training safe). 2% (2. to 3. week, p = 0. 023) and + 3.
Last Forward
Additional Information
How Does Blood Flow Restriction Therapy Work - BFR Training
Blood Flow Restriction Equipment Price - BFR Training
Bfr Training Bands Red - BFR Training
Leave a Comment:
Blog Search
Popular Blog Categories
- blood flow restriction training
- bfr training
- blood flow restriction bands
- blood flow restriction therapy
- blood flow restriction training physical therapy
- blood flow restriction physical therapy
- blood flow restriction cuffs
- blood flow restriction training for chest
- what is blood flow restriction training
- what is bfr training